







This weekend, Cape Breton-based locals 3986 and 4354 teamed up to attend strike school as bargaining continues to drag on. We’d love to conclude negotiations with a fair contract that acknowledges our hard work and pivotal role in health care, but until that happens, we’ll continue to prepare.

Can the virus live on our uniforms?
This is a common question and one of some debate since clothing can be made of many different materials and weaves. In general, viruses can live for hours or days on some surfaces, assuming it has a stable environment. Movement, friction and temperature changes can all potentially shorten the lifespan of a virus outside a human host.
To avoid contamination on clothing, health care workers should be using disposable gowns to cover their regular clothing when in contact with individuals with suspected or confirmed cases of COVID-19.
The virus is spread through respiratory droplets when an infected person sneezes or coughs. The droplets can also be spread through certain aerosol-generating medical procedures, but those would be outside the scope of practice for most home support workers.
To ensure clothing does not become infected, it’s important that we screen clients to determine if they (or anyone in the area) have symptoms, such as a fever or a new or worsening cough. If these risk factors or any others are present, use a gown.
Can the virus live on the soles of our shoes?
A recent study from the New England Journal of Medicine looked at how long the virus could live on various surfaces. It found that the virus could live for up to three days on plastics like water bottles. Given that shoes are created from various rubbers, plastics and other materials, and many are more porous than a plastic bottle, it’s reasonable to look at three days as a maximum for a surface such as a sneaker.
However, the life span of the virus is reduced by temperature changes, which would be likely to occur on a shoe people wear outside of home. While the virus living on the surface of a shoe is possible, it is not a likely source of transmission for several reasons. First, the virus is spread by respiratory droplets which would need to find their way from an infected person to a shoe. From there it would need a stable environment in order to survive, which is unlikely on a shoe as forces such as gravity will continue working on the droplets, eventually bringing them to rest on the ground. Most importantly, for the respiratory droplet to infect another person it would need to find its way from the shoe to a person’s mucus membrane, which is highly unlikely (often through the mouth, but a virus can enter through the eyes and nose as well).
What types of precautions can we take if we don’t have Personal Protective Equipment?
Personal Protective Equipment (PPE) must be used anytime we are coming into contact with an individual that is a suspected or confirmed case of COVID-19. That PPE would include a mask, gown, gloves and eye protection (face shield or goggles). There is no substitute for PPE and any members being asked to work without appropriate PPE are reminded that they have a right to refuse unsafe work. More on that here: https://cupe.ca/refusing-unsafe-work-its-your-right.
Are Home Support workers at greater risk of getting the virus because of going home to home?
The risk of contracting any infectious disease is increased in proportion to the number of people you come into contact with, so a home support worker may have more contacts than a person who is working from home but far less than someone working at the local grocery store. While all of society is working towards minimizing our contact with one another, one factor we control is our hand hygiene and use of PPE where needed.
What can we do if clients live with family? Can we asked them to go to another room?
Check with your employer for policies regarding the presence of family in your work area. To reduce the risk of exposure to an infected person, it’s important that the active screening questions are applied to anyone who will be in the home at the time the home support worker is present.
Can we leave if we are uncertain that the client is telling the truth?
Workers in Nova Scotia have the right to refuse unsafe work if they have reasonable cause to believe the work they have been assigned is likely to endanger their health and safety. More on that here: https://cupe.ca/refusing-unsafe-work-its-your-right.
When can we use the Right to Refuse?
You have the right to refuse unsafe work if you have reasonable cause to believe the work could endanger your health and safety. A work refusal, for example, might be related to PPE either not being available when needed, or being provided with PPE that you have not been trained on.
Should we be using different vehicles for work or stick with one?
How many vehicles you use is not likely to affect your likelihood of contracting a virus. Handwashing is the best defense against the spread of the virus. It’s likely that a person could touch various surfaces in their vehicle before washing their hands, creating the potential for infected respiratory droplets to be transferred to the interior of the car. This risk can be greatly reduced by washing your hands (with soap and water or hand sanitizer) before touching any surfaces.
Should we be cleaning steering wheels daily?
To reduce the chance of infection we should all be washing any surfaces in our homes and vehicles that are touched on a regular basis.
How often should I wipe off my car door handle?
Any surface you have touched after coming into contact with any surface that you didn’t clean yourself should be considered contaminated and cleaned as soon as possible. The outside door handle will be less susceptible to carrying the virus due to temperature and humidity differences; however, for an abundance of caution, it is recommended that you wipe it off anytime you touch it with hands that have not been washed.
We prepare meals for clients. Can groceries be contaminated?
Any surface that contains respiratory droplets from an infected person can be a potential source of infection. It is generally accepted that food itself is not a vector for transmission during this pandemic, but it’s not impossible for packaging to be contaminated if a sick person has coughed or sneezed on it.
To prevent the risk of infection from any surface it is highly advisable to not touch your face until you have washed your hands after touching any item or surface that you have not cleaned yourself. Good advice is to pretend everything you touch is raw chicken and wash your hands appropriately.
Would a mixture of bleach and water in a spray bottle be sufficient to clean the bottom of shoes?
Yes, bleach is an effective disinfectant when used in the proper concentrations. The CDC in the US has a good resource for identifying the best cleaning products and concentrations to use on various surfaces: https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/cleaning-disinfection.html.
What can we use for cleaning items such as phones, steering wheels and handles if Lysol wipes are not available?
The CDC resources on cleaning and disinfecting has good guidance on practices for cleaning and disinfecting various surfaces: https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/cleaning-disinfection.html.
Can we get the virus from or pass the virus to pets?
There is no evidence to suggest that pets can be infected with or be carriers for the virus. This is a pervasive myth on social media but has no scientific basis.
Does the virus live on your hair?
No studies so far have looked specifically at the ability of the novel coronavirus to live on human hair but based on available information, it’s not a likely source of transmission. Viruses tend to live longer on non-porous surfaces (like stainless steel), whereas most human hairs are quite porous and as part of a living organism, have some degree of antimicrobial properties. That being said, there is so much variety in human hair it would be a sensible precaution to wash your hair if you feel there was any chance it was exposed to someone’s respiratory droplets.
Should we shower every day after work?
If PPE is utilized when in the vicinity of suspected or confirmed cases of COVID-19 and the worker is properly trained in donning and doffing procedures, then no. That being said, no precaution is perfect, and all plans are subject to human error, so if available, a shower after work would offer an extra degree of certainty that you are not unknowingly carrying respiratory droplets somewhere on your body.
pdf format available here: Q&A.HOME.SUPPORT.APR.1
Infection Prevention & Control Guidelines within Home Care & Community Care Settings
The current outbreak of coronavirus disease (COVID-19) is caused by a newly identified virus, the SARS coronavirus2 (SARS-CoV-2). Most people with COVID-19 have only mild symptoms and do not require admission to hospital. However, some have developed severe illness and deaths have been reported. There is evidence that COVID-19 can be spread from people who are sick to others with whom they have close contact. Close contact involves situations such as caring for, or living with someone who is ill.
Organizations, agencies, and individuals that provide health care to clients in their home/community setting need to be prepared to look after individuals with COVID-19 (suspected and confirmed). The guidance in this document is intended for care providers who see clients in their home/community setting. It will be updated as new information becomes available.
Screening and Triage Home Care and Community Care services will conduct passive and active screening of clients and their families. Passive screening for clients and their families All clients should be asked to report fever > 38 degrees Celsius and/or new or worsening cough in themselves or a household member to the Home Care and Community Care services provider before the visit at a number provided to them. Active screening for clients and their families
All clients and their household members should be screened for COVID-19 by a designated staff member (e.g., continuing care assistant, nurse, scheduler, manager, and other health care professionals) by phone the day of the scheduled visit. The following screening questions should be asked of client and household members: Do you have?
1. Fever (temperature over 38 degrees Celsius) OR symptoms of a fever (no thermometer available) AND/OR new onset or worsening of chronic cough
AND any of the following:
2. Travel outside of Canada in the 14 days before the onset of illness OR close contact with a confirmed or probable case of COVID-19 OR close contact with a person with acute respiratory illness who has been outside of Canada in the 14 days before their symptom onset. NOTE: Screening questions are subject to change through direction of the office of the Chief Medical Officer of Health, DHW. Staff should also ask if other people will be in the home during the appointment (e.g. nonhousehold visitors) and ask them the screening questions as well. Clients, household members, and/or non-household visitors in the home who answer yes to screening questions 1 and 2 should be directed to contact 811 for advice on the most appropriate setting for clinical assessment and testing (if warranted).
If the client or household member states that they are very ill, the staff person should advise the client/household member to contact 911 (EHS) as they may require emergent care. If the client and/or household member is suspected to have or has tested positive for COVID-19 and is self-isolating or recuperating at home:
• Necessary client care will continue using the infection prevention and control guidance as below.
• All Non-Urgent care should be postponed. Examples: Can non-essential housekeeping be postponed until the client does not require additional precautions? Can physiotherapy or occupational therapy be postponed until the client does not require additional precautions? Can non-urgent care coordinator assessments or reassessments be postponed until the client does not require additional precautions? Conduct assessments (e.g. care coordination) via phone as much as possible.
Infection Prevention & Control Guidance for Caring for a Client with Suspected or Confirmed COVID-19
Care providers will, in addition to Routine Practices, implement Droplet & Contact Precautions and use the correct personal protective equipment when within 2 metres of the client. *In some circumstances the client may not be a suspected or confirmed case, but a member of the household/family member is. Any symptomatic people in the household should be asked to remain in another room during the visit. Droplet and Contact Precautions should still be initiated.
Routine Practices
Routine Practices should be consistently used with all clients. The key to implementing Routine Practices is for care providers in home care/community settings is to conduct a Point of Care Risk Assessment (PCRA) with each client interaction. The PCRA will assess risk of transmission of microorganisms and assist staff to choose interventions or infection control measures to use. This includes assisting the health care worker to select the appropriate personal protective equipment (See Appendix A).
Droplet & Contact Precautions
For cases of suspected or confirmed COVID-19, Additional Precautions (Droplet and Contact) will be implemented. Droplet and Contact Precautions include:
• Ensuring that for any visit, the health care worker has the appropriate supplies, including personal protective equipment (PPE), to make certain that the additional precautions are maintained.
• Ensuring the home/community setting has a safe place to put on and remove PPE.
• Performing Hand Hygiene, with an alcohol-based hand rub or soap and water, whenever indicated (Four Moments of Hand Hygiene), paying particular attention to during and after removal of PPE, and after leaving the client care space.
• Dedicating client care equipment or ensuring all equipment (e.g. stethoscope) is cleaned and disinfected between clients with a hospital-grade disinfectant/wipe. If paper forms must be completed and signed by the client: use a disposable pen that can be left in the home and use a plastic clipboard that can be wiped down with disinfectant. The papers can be placed in a folder and usual processes followed.
• Cleaning of the client care environment using a disinfectant wipe as necessary. Attention should be paid to high touch surfaces.
• Using appropriate personal protective equipment (PPE) for Droplet and Contact precautions. This includes gloves, long-sleeved gown, procedure/surgical mask and eye/face protection.
• Avoiding doing aerosol-generating medical procedures (AGMPs) in the home. Alternative therapy should be explored when possible including use of alternatives such as meterdosed inhaler with spacer instead of nebulizer. If an AGMP (e.g. nebulized therapy) is necessary and unable to be administered by the client or household member, it should be administered by nursing staff trained in the use of Additional Precautions. A fit tested respirator (N95) is required in addition to Droplet and Contact precautions. The respirator is not removed until after leaving the client’s home.
• Ensuring proper training in putting on and removing PPE in order to prevent crosscontamination and the potential spread of infection (refer to attached NSHA signage in Appendix B & C) and the following video.
After applying the required PPE, the care worker should instruct the client to wear a procedure mask (if tolerated) while the care worker is providing care. Clients should also be instructed on respiratory/cough etiquette including sneezing/coughing into their elbow or tissue, putting used tissues into a waste receptacle and performing hand hygiene immediately following.
The duration of Droplet and Contact Precautions should be determined in consultation with Public Health.
Household members, family members, private caregivers who are also involved in caregiving for the client can be directed to the following Public Health Agency of Canada webpage: Coronavirus disease(COVID-19): How to care for a person with COVID-19 at home- Advice for caregivers. It offers advice on preventative measures that can be utilized in the home environment.
Employee Health
• Care providers who become ill with a respiratory infection should report their illness to their organization and follow established protocols. • If COVID-19 is suspected or diagnosed in a care provider, case management and return to work should be determined in consultation with local public health/Medical Officer of Health. Ill care providers should not work at any healthcare facility or organization until cleared to return to work.
Specimen Collection and Testing
At this time, home and community care providers are not expected to conduct testing for COVID19. All health care providers have a duty to report a client who has or may have COVID-19 to their local Public Health Offices. The care provider should refer them to 811 for the most appropriate setting for the client to be clinically assessed and tested.
For more information:
NSHA Coronavirus Disease (COVID-1) webpage Nova Scotia Department of Health and Wellness Novel coronavirus (COVID-19) webpage
References: Nova Scotia Department of Health. Coronavirus Webpage. Ontario Ministry of Health. Novel Coronavirus (COVID-19) Guidance for Home and Community Care Providers. (February 11, 2020). Public Health Agency of Canada (2020). Infection Prevention and Control for COVID-19: Interim Guidance for Acute Healthcare Settings
Province of Nova Scotia. (2019). Respiratory Response Plan for Public Health (including SARI, novel influenza and novel coronaviruses) 2019-2020. Province of Nova Scotia. (2020). Nova Scotia Interim Guidance: Public Health Measures of cases and contacts associated with Novel Coronavirus (COVID-19). Date: March 4, 2020
Appendix A- Point of Care Risk Assessment (PCRA) Point of Care Risk Assessment
Before each patient/resident/client interaction, the health care worker completes a ‘Point of Care Risk Assessment’ (PCRA) by asking the following questions to determine the risk of exposure and appropriate Routine Practices and Additional Precautions required for safe care:
• What are the client’ symptoms?
• What is the degree of contact?
• What is the degree of contamination?
• What is the client’s level of understanding and cooperation?
• What is the degree of difficulty of the procedure being performed and the experience level of the care provider?
• What is my risk of exposure to blood, body fluids, excretions, secretions, non-intact skin and mucous membranes?
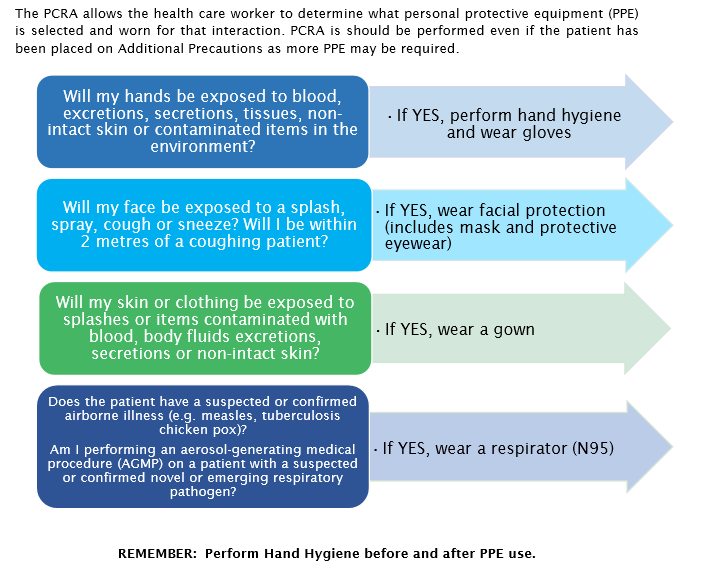
The PCRA allows the health care worker to determine what personal protective equipment (PPE) is selected and worn for that interaction. PCRA is should be performed even if the patient has been placed on Additional Precautions as more PPE may be required.


Information to Continuing Care Sector
COVID-19 FAQ
1. I have employees who returned from travel outside of Canada BEFORE March 13, 2020. Should these employees be directed to self isolate?
No, however employees who returned from travel outside of Canada BEFORE March 13, 2020 are expected to closely monitor their health. If the employee begins to experience symptoms (fever, new cough, or difficulty breathing), they are required to self-isolate and call 811 for direction. More information on when you should call 811 can be found at: https://811.novascotia.ca/health_topics/covid-19-when-to-call-811/
2. I have employees who returned from travel outside of Canada AFTER March 13, 2020. Should these employees be directed to self isolate?
Yes. Employees who returned from travel outside of Canada AFTER March 13, 2020 have been directed to self-isolate for fourteen days. They should not come to work. Employees who have been directed to self-isolate should be paid during their self-isolation. Please track these costs and report them to the department through the financial impact reporting process.
3. I have an employee in home care/long term care who lives with someone who has been directed to self-isolate for 14 days. Can they still work?
Yes, employees who live with someone who has been directed to self-isolate should report to work. If the traveller develops symptoms, they should call 811 to be assessed for testing, and the employee should self-isolate and closely monitor themselves for symptoms until it is determined whether or not the traveller tests positive for COVID19. Individuals who are self-isolating should limit contact with household members. Visit www.novascotia.ca/coronavirus for more information on self-isolation.
4a. Can nursing home residents continue to go into the community to visit friends and family?
There are no government restrictions on residents leaving facilities. This should be determined on a case-by-case basis in cooperation with the resident. Considerations include where the resident will be going and their ability to adhere to respiratory etiquette, hand hygiene practices and understanding of social distancing (staying two meters or 6 feet apart from others).
March 17, 2020
COVID-19 FAQ (CONTINUED)
4b. If yes, how should staff support this? If outings are approved following a case-by-case assessment, staff should remind the resident about the importance of social distancing, practicing respiratory etiquette and good hand hygiene. Within the facility, staff can ensure high touch surfaces are cleaned and disinfected frequently to minimize the potential of the spread of illness.
5. Should residents be isolated upon return from an outing in the community?
It is not necessary to isolate residents after leaving the facility unless the resident has: a) travelled outside of Canada, or b) been in contact with someone who is experiencing symptoms and has travelled outside of Canada, or c) been in contact with someone who has a presumptive positive diagnosis of COVID19
6. I have a resident who leaves long term care three times per week for dialysis. Should that resident be isolated upon return from dialysis?
That is not necessary. The resident should be encouraged to follow the advice provided for all Nova Scotians to practice social distancing as much as possible, respiratory etiquette, and good hand hygiene by washing hands with soap and water and/or using hand sanitizer often.
7. Should home support and home care staff be leaving their work cell phone in their vehicle so that they don’t bring germs in and out of home support client homes?
That is not necessary, but phones and other frequently touched handheld devices should be cleaned and disinfected between clients, using appropriate disinfectant wipes.
novascotia.ca/coronavirus
We have been hearing a lot from our home support members who have questions about how COVID-19 affects their work and about their personal safety. We hope the following will answer some of those questions.
The Precautionary Principle
Knowledge about how the virus is transmitted has yet to be fully understood. For this reason, CUPE is recommending that health care settings adopt the precautionary principle towards infection prevention and control of COVID-19. The precautionary principle means taking action to prevent infection from potentially serious viruses without having to wait for complete scientific proof that a course of action is necessary. While there is continued uncertainty that the virus is not spread through the air, we must conduct ourselves as if it were.
How is the Virus Spread?
The prevailing consensus among health agencies including the Public Health Agency of Canada (PHAC), Center for Disease Control (CDC) and the World Health Organization (WHO) is that the virus is spread primarily through close contact (within two metres) with an infected person through respiratory droplets generated when a person, for example, coughs or sneezes, or through droplets of saliva or discharge from the nose.
There remains no consensus if COVID-19 is transmitted by small droplets suspended in the air or through procedures that generate aerosols (e.g open suctioning). As such, CUPE is recommending that workers and employers treat COVID-19 as an airborne transmitted disease.
What is the Incubation Period?
The prevailing consensus is that time between infection and the onset of clinical symptoms of the disease is 1 -12 days. Coronaviruses have incubation periods that can last up to 14 days. As such, CUPE recommends that health care settings adopt a more conservative incubation period of greater than 14 days without symptoms.
Can the Virus be Spread by a Person with no Symptoms of the Disease (Asymptomatic)?
There is no consensus that an asymptomatic person can not transmit the disease during the incubation period. In rare cases, transmission of the virus has occurred from an asymptomatic person. For this reason, CUPE is recommending that health care settings adopt the precautionary principle until it is fully understood how the virus is transmitted.
This means that members of a community who have had contact from a person who has developed COVID-19 but has not shown symptoms, should be treated as if they carry the virus.
Advice to CUPE Locals:
CUPE has been receiving many questions from members who want to know how the current COVID-19 pandemic may affect their right to refuse. As a worker in Nova Scotia, you have the legal right to refuse unsafe work, according to Section 43 of the Occupational Health and Safety Act, when there are reasonable grounds to believe that the work condition, equipment, material, or any aspect of the work may be dangerous to you or another person’s health and safety.
Here’s how you can refuse unsafe work:
You cannot be threatened or discriminated against through dismissal, reprimand or reduction of either wages or benefits for complying with the legislation, according to Section 45 of the Act.
How does COVID-19 effect the potential that an aspect of the work may be dangerous to the workers’ health and safety?
For employees who are not working with people who are ill or showing symptoms of illness (such as fever and a cough) COVID-19 is not a significant risk to a worker. While the risk to public health remains high, the risk to the health and safety of individual workers is not significantly impacted at this time. The ability to evoke your right to refuse is individual and based on your own assessment of the risk. Consider factors such as ability to maintain hand hygiene and a safe distance from anyone who is exhibiting symptoms.
How does COVID-19 affect the potential that an aspect of the work may be dangerous to the workers’ health and safety when working with people who are infected or showing symptoms of illness?
If you work in health care or any sector that brings you into contact with individuals who are ill or suspected to be ill, ensure you are familiar with your employer’s infection prevention and control procedures. If you lack the training, staffing levels, or personal protective equipment they call for to perform the tasks you have been assigned, please take those factors into consideration when evaluating the risks. As always, the determination that a situation is dangerous is an individual one and the role of your union is to ensure members are aware of their rights and the processes to follow.
It is also important to remember that the efforts to enhance health and safety in your workplace are always ongoing, and any situation that can affect the health and safety of any person in the workplace should be reported immediately to a supervisor.
To run our online services, such as web-based email, web hosting, and online campaigns, we need to be able to check to see that our users are who they say they are. That means collecting personal information like names, postal codes and phone numbers. We acknowledge that this is important, personal information and we acknowledge the responsibility that comes with it. We take your privacy seriously.
We will never sell, trade, rent or donate any information you give us.
We honour all unsubscribe requests, whether automatically or by email to cupehome@gmail.com.
None of our interactive services display your email address publicly.
When you participate in our online actions, we will collect your email address and store it securely.
We will contact you by email about CUPE initiatives, as well as social justice and political action campaigns.

Many workers are placed at risk because they are required to work alone.
CUPE defines working alone to mean working at a worksite for any period of time as the only worker, where assistance is not readily available in the event of injury, ill health or emergency.
When working alone, a worker has no ability to call for help if incapacitated by an unexpected incident or emergency. When working alone, competent supervision and guidance is not present to ensure that appropriate controls are in place and safe procedures followed.
Many CUPE members are put at risk because employers have no policy or procedures that recognize and seek resolutions to the problem of working alone.
Many jobs require two people to be done safely. When a worker is alone in jobs where exposure to a serious hazard is part of the working conditions, there is a greater chance of serious injury. A worker can also be denied help or assistance and as a result, may suffer further injury or death. Hazards that make working alone particularly dangerous include tasks that put the worker at risk of
Employers are legally obligated to provide a healthy and safe workplace. As of January 2014, Alberta, British Columbia, Manitoba, New Brunswick, Quebec, Saskatchewan, Newfoundland and Labrador, and Prince Edward Island all have specific legislation in the occupational health and safety acts that deals with working alone. Though the federal jurisdiction, Ontario, and Nova Scotia don’t have specific provincial legislation, government policies and procedures are widely understood to mean that working alone is a hazard to be protected against under the general duty clause.
Please check your provincial health and safety act and regulations for specific legislative requirements in your province.
The first step is to identify tasks that require workers to work alone. To identify these tasks, members can use the survey in the CUPE Working Alone Guidelines, which can be ordered online at cupe.ca/health-and-safety. It is preferable to proceed with buy-in and cooperation from the employer, however if support is not forthcoming, locals should conduct the survey on their own. Once completed, the survey results can help pinpoint potential problem jobs and act as a basis for recommendations to the joint health and safety committee or to the employer.
Recommendations can include:
A) Developing or re-examining employer policies regarding working alone. The policy should list all tasks with inherent dangers that should never be conducted alone, and ensure sufficient staff are available to enforce the policy. The policy should also instruct members not to attempt to perform work identified as hazardous without the assistance of a second person.
B) Developing written procedures covering dangerous work situations:
C) Education and training requirements ensuring all workers fully understand the policy and procedures. The education and training must also ensure workers are fully trained to recognize and deal with the hazards they face in their work. Training must be offered to all new employees, and updates to training must be provided for all workers on a regular basis.
This fact sheet is part of a more detailed CUPE guideline on working alone. Order the full guideline online at cupe.ca/health-and-safety.
For more information contact:
CUPE National Health and Safety Branch
1375 St-Laurent Boulevard
OTTAWA, ON K1G OZ7
Tel: (613) 237-1590
Fax: (613) 237-5508
Email: health_safety@cupe.ca